
Thoracic Outlet Syndrome (TOS): A Practical, Evidence-Informed Overview
What is Thoracic Outlet Syndrome?
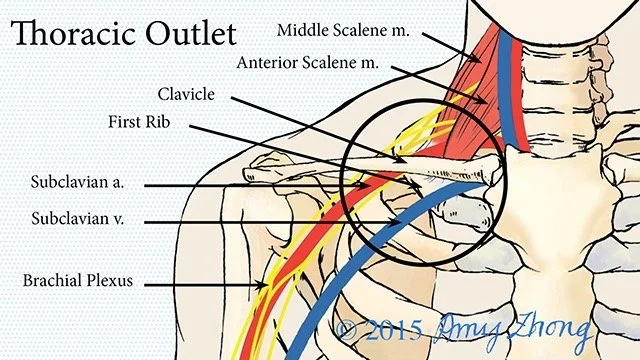
Thoracic Outlet Syndrome (TOS) refers to a group of conditions involving compression, irritation, or increased sensitivity of the neurovascular structures that travel from the neck into the arm, primarily the brachial plexus, subclavian artery, and subclavian vein.
While often simplified as a “compression problem,” current evidence suggests that many presentations, particularly neurogenic TOS, involve a combination of mechanical sensitivity, load intolerance, and nervous system irritability, not just structural narrowing.
Key Anatomical Regions
The term “thoracic outlet” doesn’t refer to a single structure, but rather a series of anatomical spaces:
Interscalene Triangle
Between the anterior and middle scalene musclesCostoclavicular Space
Between the clavicle and first ribSubcoracoid (Retropectoralis Minor) Space
Beneath the pectoralis minor tendon
These are common sites where symptoms may be provoked, though identifying a single “point of compression” is not always possible.
Types of TOS
• Neurogenic TOS (≈90–95% of cases)
• Venous TOS (e.g., effort thrombosis / Paget-Schroetter syndrome)
• Arterial TOS (rare, but more serious)
“Non-specific” or “disputed” TOS remains debated and is increasingly being reframed in terms of pain science and peripheral nerve sensitivity.
Symptoms
Symptoms can vary widely and often overlap with other conditions.
Common patterns include:
• Neck, shoulder, and arm pain
• Paresthesia (tingling, numbness, burning)
• Hand weakness or fatigue
• Cold sensitivity or vascular changes
• A sense of heaviness or poor endurance in the arm
A key clinical feature is that symptoms are often position-dependent, especially with overhead or sustained arm use.
Causes & Contributing Factors
TOS is rarely caused by one single factor.
Instead, it tends to emerge from a combination of:
• Repetitive strain or sustained positioning
• Trauma (e.g., whiplash injuries)
• Sudden increases in training or workload
• Anatomical differences (less common, but relevant)
• Deconditioning or reduced tissue capacity
Posture is often overemphasized, and while it can influence symptoms, it is not considered a primary driver in most cases.
Diagnosis
There is no single definitive test for most forms of TOS.
Diagnosis relies on:
• Clinical reasoning
• Symptom behaviour
• Physical examination findings
Imaging is typically reserved for:
• Suspected vascular involvement
• Severe or progressive neurological findings
Treatment: What Actually Helps?
Conservative care is the primary approach.
An evidence-informed plan typically includes:
1. Education
Understanding the condition reduces fear and improves outcomes
2. Symptom Modulation
Manual therapy, movement, and load management
3. Progressive Loading
Gradual strengthening of the shoulder girdle and neck
4. Movement Retraining
Improving tolerance to daily and occupational demands
5. Pacing & Activity Modification
Reducing flare-ups while maintaining function
When is Surgery Considered?
Surgical intervention may be appropriate in cases of:
• Confirmed vascular compromise
• Progressive neurological deficit
• Failure of well-managed conservative care
Final Thoughts
TOS can be frustrating, both for patients and clinicians, because it doesn’t always present clearly or respond quickly.
But with the right approach, many people see meaningful improvement.
If your symptoms don’t quite fit a typical “neck” or “shoulder” pattern, it may be worth a closer look.